What is an SBAR in nursing
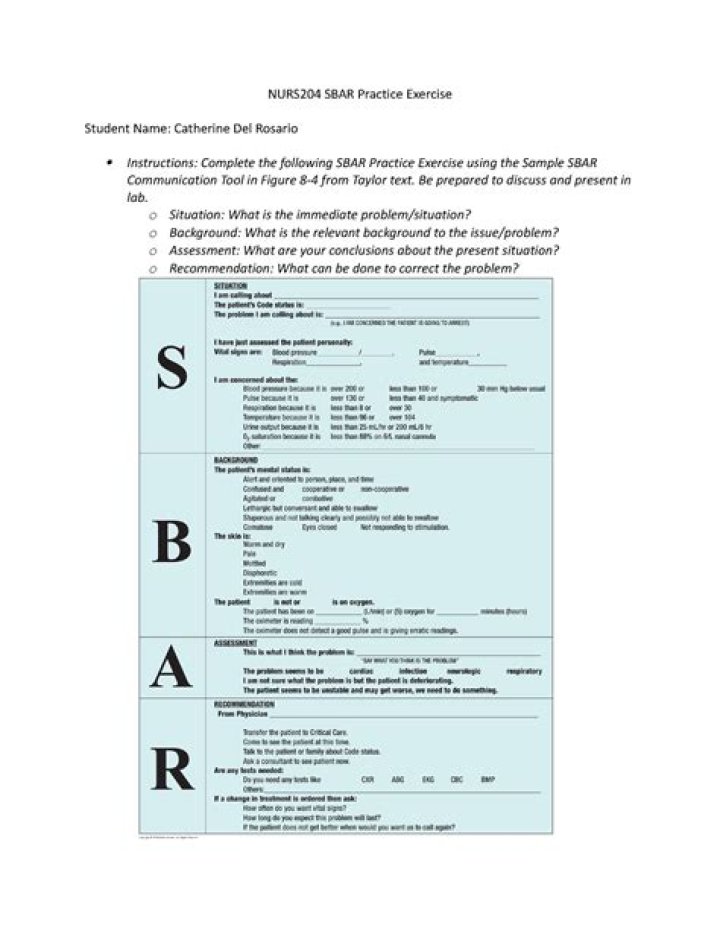
Communicating with SBAR. The SBAR (situation, background, assessment and recommendation) tool is provided below to aid in facilitating and strengthening communication between nurses and prescribers throughout the implementation of this quality improvement initiative.
What is an example of SBAR?
Safer Healthcare provides the following example of SBAR being used in a phone call between a nurse and a physician: “Dr. Jones, this is Deb McDonald RN, I am calling from ABC Hospital about your patient Jane Smith.”
What information should be included in SBAR?
This includes patient identification information, code status, vitals, and the nurse’s concerns. Identify self, unit, patient, room number. Briefly state the problem, what is it, when it happened or started, and how severe.
What is the SBAR tool used for?
SBAR Tool: Situation-Background-Assessment-Recommendation. The SBAR (Situation-Background-Assessment-Recommendation) technique provides a framework for communication between members of the health care team about a patient’s condition.What is SBAR template?
SBAR is an acronym for Situation, Background, Assessment, Recommendation. It is a technique used to facilitate appropriate and prompt communication. An SBAR template will provide you and other clinicians with an unambiguous and specific way to communicate vital information to other medical professionals. Advertisements.
What is iSoBAR handover and why is it necessary?
Use of structured handover tools can help to provide a framework for communicating the minimum information content for clinical handovers. The iSoBAR framework is an example. A ‘patient safety check’ process at the end of a handover can help to focus on the patient’s safety as a priority.
What is an SBAR handover?
The communication tool SBAR (situation, background, assessment and recommendation) was developed to increase handover quality and is widely assumed to increase patient safety. … Primary and secondary outcome measures Aspects of patient safety (patient outcomes) defined as the occurrence or incidence of adverse events.
How long should an SBAR be?
It is recommended that this element be brief and last no more than 10 seconds. It is recommended that health care professionals identify the person with whom they are speaking, to introduce oneself (including title or role) and where one is calling from.What elements are included in a pain assessment?
Patients should be asked to describe their pain in terms of the following characteristics: location, radiation, mode of onset, character, temporal pattern, exacerbating and relieving factors, and intensity. The Joint Commission updated the assessment of pain to include focusing on how it affects patients’ function.
What is the first step in the SBAR communication technique?Each component of SBAR—situation, background, assess- ment, recommendation—provides a format for which to present information in a specific, organized way. The first step of the SBAR tool is stating the situation. In other words, what is the problem?
Article first time published onWhen should a nurse use sbar?
- Conversations with physicians, physical therapists, or other professionals.
- In-person discussions and phone calls.
- Shift change or handoff communications.
- When resolving a patient issue.
- Daily safety briefings.
- When you’re escalating a concern.
- When calling an emergency response team.
How do I write a good bedside report?
- Give a Bedside Report. “Check pertinent things together such as skin, neuro, pulses, etc. …
- Be Specific, Concise and Clear. “Stay on point with the ‘need to know’ information. …
- When in Doubt, Ask for Clarification. …
- Record Everything. …
- Be Positive!
How do you make a report?
- Decide on terms of reference.
- Conduct your research.
- Write an outline.
- Write a first draft.
- Analyze data and record findings.
- Recommend a course of action.
- Edit and distribute.
What should a handover nurse include?
- Past: historical info. The patient’s diagnosis, anything the team needs to know about them and their treatment plan. …
- Present: current presentation. How the patient has been this shift and any changes to their treatment plan. …
- Future: what is still to be done.
How do I write an iSoBAR?
The acronym “iSoBAR” (identify–situation–observations–background–agreed plan–read back) summarises the components of the checklist.
What does SBAR stand for in healthcare?
The SBAR (situation, background, assessment and recommendation) tool is provided below to aid in facilitating and strengthening communication between nurses and prescribers throughout the implementation of this quality improvement initiative.
How do you write a soapie note?
- Summarize subjective information. Record subjective information about the patient’s experience in the first section of the SOAPIE note. …
- List objective data. …
- Complete a patient assessment. …
- Outline the treatment plan. …
- Describe healthcare interventions. …
- Evaluate the interaction.
What does Idraw stand for?
The acronym IDRAW was developed to provide a template or framework on which to structure an efficient and effective verbal patient handover. IDRAW stand for Identify Patient & MRP, Diagnose Current Problems, Recent Changes, Anticipated Changes, What To Watch For.
What is the Aidet model?
The acronym AIDET® stands for five communication behaviors: Acknowledge, Introduce, Duration, Explanation, and Thank You. … It’s a simple, consistent way to incorporate fundamental patient communication elements into every patient or customer interaction.
What does R stand for in Isbar?
It stands for Introduction, Situation, Background, Assessment and Recommendation.
How do I write an Isbar handover?
Using ISBAR for verbal/written communication (e.g. phone call, email or referral) Identify: yourself and your role, and the patient/resident using the three patient identifiers (name, date of birth (DOB) and UR number). Refrain from referring to the patient by their location “the patient in bed 5”.
What are the 4 types of pain?
- Nociceptive Pain: Typically the result of tissue injury. …
- Inflammatory Pain: An abnormal inflammation caused by an inappropriate response by the body’s immune system. …
- Neuropathic Pain: Pain caused by nerve irritation. …
- Functional Pain: Pain without obvious origin, but can cause pain.
What does Pqrst mean in nursing?
The mnemonic device PQRST offers one way to recall assessment:P. stands for palliative or precipitating factors, Q for quality of pain, R for region or radiation of pain, S for subjective descriptions of pain, and T for temporal nature of pain (the time the pain occurs).
What should a nurse document regarding a patient's pain?
It is important to document the following: Patient’s understanding of the pain scale. Describe the patient’s ability to assess pain level using the 0-10 pain scale. Patient satisfaction with pain level with current treatment modality.
What are the disadvantages of sbar?
Limitations of SBAR tool The SBAR tool requires training of all clinical staff so that communication is well understood. It requires a culture change to adopt and sustain structured communication formats by all health care providers.
Which communication technique is nontherapeutic?
Sympathy is the nontherapeutic communication technique exhibited by the nurse in this scenario. Sympathy is concern, sorrow, or pity felt for another person. Sharing humor is a therapeutic communication technique.
When should the rapid response team not be called?
Respiratory rate over 28/min or less than 8/min. Systolic blood pressure greater than 180 mmHg or less than 90 mmHg. Oxygen saturation less than 90% despite supplementation. Acute change in mental status.
Which nurse would most likely be the best communicator?
Which of the following nurses most likely is the best communicator? A nurse who easily developed a rapport with clients.
Does SBAR improve communication?
Published evidence shows that SBAR provides effective and efficient communication, thereby promoting better patient outcomes.
Which of the following statements describes the purpose of the nursing process?
Which of the following statements describes the purpose of the nursing process? … The nursing process is a way to systematically think about and use patient data.